Interventional Pulmonology Services
 Interventional pulmonology is a growing area of pulmonary medicine that
uses state-of-the-art, minimally invasive procedures to diagnose and treat
diseases of the lung and membranes around the lungs (pleurae).
Interventional pulmonology is a growing area of pulmonary medicine that
uses state-of-the-art, minimally invasive procedures to diagnose and treat
diseases of the lung and membranes around the lungs (pleurae).
The Interventional Pulmonology Service (IPS) at Robert Wood Johnson University Hospital — in partnership with Rutgers Group — offers inpatient and outpatient services to treat both benign and malignant diseases in adults.
 Our
expert team collaborates closely with the
Thoracic Surgery,
Medical Oncology, Radiation Oncology and Interventional Radiology departments to provide individualized, integrated care.
Our
expert team collaborates closely with the
Thoracic Surgery,
Medical Oncology, Radiation Oncology and Interventional Radiology departments to provide individualized, integrated care.
To maximize a patient’s time away from the hospital, decrease cost and facilitate access to health care, IPS offers minimally invasive procedures for the diagnosis and symptomatic relief of dyspnea, or shortness of breath, associated with benign and malignant pleural effusions through the outpatient clinic.
Our Programs
Pleural Effusion Management
Pleural effusion is fluid buildup in the space between the two layers of tissue that line the lungs and the chest wall. There is usually a small amount of fluid that exists to help the lung to move easily when breathing. However, when a person has excessive fluid accumulation, the lung(s) will be displaced, compromising function and causing them to feel short of breath and/or experience chest pain. The procedures outlined below can be done individually or together — depending on the person's condition — to relieve their symptoms. Some of them can even be performed in an outpatient setting.
-
Thoracentesis
Thoracentesis is a procedure in which the area of the chest wall is anesthetized prior to inserting a needle into the pleural space between the lung and wall to remove excess fluid. It may be performed in both the inpatient and outpatient settings. -
Indwelling Pleural Catheter Placement
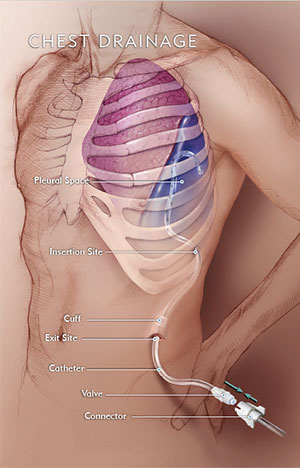
A thin, flexible tube, or catheter, can be inserted from outside of the chest into the lung to drain excessive fluid buildup. A patient may have this catheter inserted in an outpatient setting and return home the same day, avoiding the need for repeated, uncomfortable injections and chest tubes as well as multiple trips to the hospital or the outpatient service. The patient is in control of draining the fluid through this special catheter, which has an easy-to-access valve that rests outside the chest wall. -
Pleurodesis
Pleurodesis is a procedure that uses a special talc to help the lungs stick to the chest wall, and can be done both in the inpatient and outpatient setting. If doctors find that there is repeated buildup of fluid or air between the lungs and the chest wall, or if a patient's lung repeatedly collapses, a pleurodesis can be done at the same time as a medical thoracoscopy. -
Medical Thoracoscopy
With just a small incision through the chest wall, this minimally invasive technique is used to evaluate excessive, recurring fluid buildup between the membranes that line the lungs. During this procedure, the lung is intentionally collapsed to obtain fluid and tissue biopsies to be evaluated in real-time by pathologists so that any further problems discovered by the interventional pulmonologist may be addressed immediately. A chest tube is then inserted to re-inflate the lung. Once confirmed by chest x-ray, the chest tube is removed and the patient is discharged.
Bronchoscopic Lung Volume Reduction
The Bronchoscopic Lung Volume Reduction (BLVR) program is for patients with chronic obstructive pulmonary disease (COPD) and lung hyperinflation. The goal is to reduce hyperinflation or shortness of breath and improve the patient’s quality of life. Once a patient is identified as a candidate for BLVR, the interventional pulmonologist will place one-way valves into the affected airway. This is called endobronchial valve placement.
Interstitial Lung Disease Management
Interstitial lung disease (ILD) occurs when the air sacs in the lungs are damaged because of environmental factors or a family history of the disease. This damage causes the lungs to become stiff, which makes it difficult to breathe and get oxygen to circulate through the bloodstream. To diagnose a patient with ILD, interventional pulmonologists conduct pulmonary function tests, review imaging, and use diagnostic bronchoscopy to view and sample the lung tissue. Patients with ILD will need continual follow-up to manage their disease.
Management of Tracheoesophageal Fistula
A tracheoesophageal fistula is an abnormal connection or passageway that occurs when the lining between the trachea and the esophagus becomes compromised due to certain cancers or pressure ulcers from tracheostomies. In conjunction with advanced gastrointestinal physicians, interventional pulmonologists will visualize the airway with a bronchoscope and depending on the location of the fistula, will either place a covered stent or suture the fistula closed.
Procedures We Perform
Diagnostic Bronchoscopy
Diagnostic bronchoscopy enables the interventional pulmonologist to visually inspect the airways. A fiberoptic scope is used along with specialized tools and equipment to assess the openness of the airways. It also makes it easier for the interventionalist to find ideal spots in affected areas of the lungs from which to obtain tissue samples. We use state-of-the-art bronchoscopic technology and methods to perform these diagnostic bronchoscopies:
-
Functional Bronchoscopy
Patients with chronic cough and/or shortness of breath may need to be evaluated for excessive dynamic airway collapse (EDAC), a narrowing or possible collapse of the airway during breathing. Functional bronchoscopy is a procedure performed by the interventional pulmonologist using a fiberoptic scope while a patient is under moderate sedation to visually inspect the trachea, assess whether there is potential for airway collapse, and establish the severity. The results of this test will determine whether further therapeutic interventions are necessary, such as airway stenting, continuous positive airway pressure (CPAP) therapy, or surgery. -
Parenchymal Cryobiopsy
Parenchymal (interstitial) lung disease can occur due to any number of factors: infection, environmental exposure, malignancy, drugs, or other unknown causes. A patient may have shortness of breath, cough, weight loss, fever, skin rashes, or in some cases no symptoms at all. To determine treatment options for the patient, tissue samples must be obtained and evaluated. A bronchoscopy is performed and a tiny probe is inserted into the affected lung. The tissue is frozen and extracted through the scope, this is called a parenchymal cryobiopsy. This minimally invasive technique allows the interventional pulmonologist to obtain larger, better preserved tissue samples of the lungs, allowing for improved diagnosis.
Therapeutic Bronchoscopy
In therapeutic bronchoscopy, the interventional pulmonologist visually inspects the airways and performs procedures to relieve the patient’s symptoms. Usually the patient is discharged the same day. These procedures include:
-
Rigid Bronchoscopy
Specialized equipment is used to remove large foreign bodies in the airway, place a silicone stent in the main bronchus, perform rapid mechanical debulking of a tumor, dilate a narrowed (stenotic) airway, or control large-volume airway hemorrhages. -
Tumor Debulking
Using cryotherapy — the freezing and removal of tissue — and/or argon plasma coagulation (APC) — a specialized probe with the argon gas that destroys the invasive tissue— interventional pulmonologists can remove excess tissue causing obstruction of the airways. -
Tracheobronchial Stenting
In this procedure, a variety of different stents (silicone stents, fully and partially covered and uncovered) can be used to maintain openness of the airway due to obstructions. -
Bronchial Thermoplasty
This procedure employs a device that delivers controlled, localized radiofrequency waves, or heat, to the airways during bronchoscopy, which reduces the increased mass of airway smooth muscle associated with asthma.


