Therapeutic Endosonography
EUS-guided celiac plexus block and celiac plexus neurolysis
Patients with intractable pain from chronic pancreatitis or pancreatic cancer can benefit from a celiac plexus block or celiac plexus neurolysis. The procedure involves using Endoscopic Ultrasound to identify the celiac plexus, a block of nerves that are responsible for pain from the pancreas. This block of nerves is then injected with an anesthetic agent to deaden the nerves either temporarily (block) or permanently (lysis). The procedure is performed endoscopically, with sedation similar to what is given during a routine colonoscopy.
EUS-guided fiducial placement
Many patients with cancer of the gastrointestinal tract will receive radiation as part of their therapy. This procedure includes identifying the tumor via Endoscopic Ultrasound. Once identified, small gold cylinders, called fiducials, are endoscopically implanted around the borders of the tumor. The fiducials are then identified radiographically, which allows for precise application of radiation to the desired location.
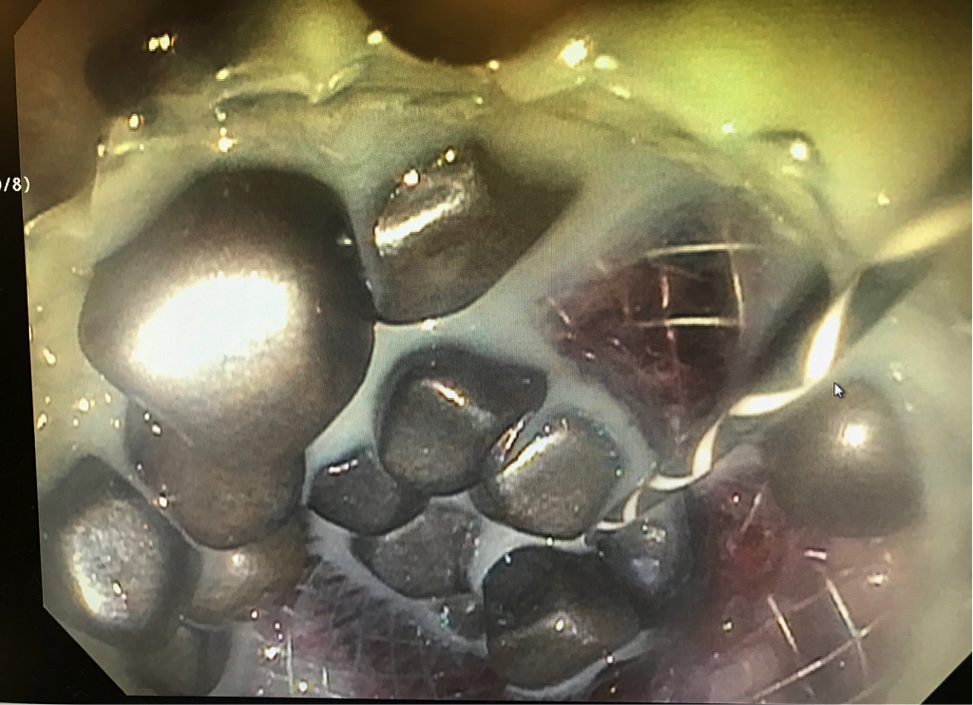
EUS-guided glue and coils injection
Patients with end-stage liver disease, called cirrhosis, are at risk for development of dilated blood vessels in the stomach, called gastric varices. These blood vessels are at high risk for causing major bleeding into the stomach. One novel approach to management of this type of bleeding is to inject a type of glue with a metal coil into the vessel, which causes it to harden and decreases the chance of bleeding.
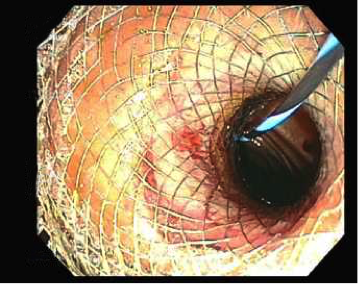
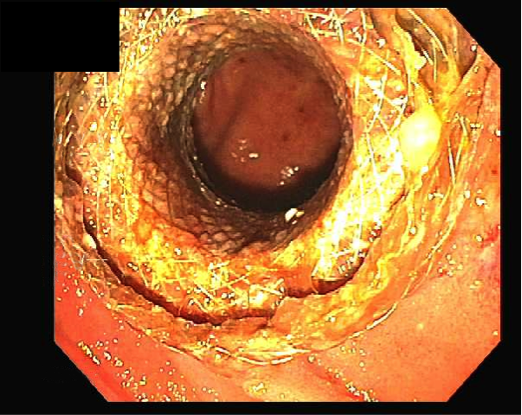
Endoscopic transmural drainage of pseudocyst and abscesses
Approximately 5-15% of patients with pancreatitis, or inflammation of the pancreas, will develop a walled off collection of fluid, called a pancreatic fluid collection. These collections can be painful and/or become infected, in which case drainage of the collection is required. Traditionally, these collections required drainage via surgery or a tube inserted through the skin, but now we have the capability to drain them from the inside, without the need for external tubes or incisions. Your doctor can see the collection using Endoscopic Ultrasound and place a stent from the collection into the lumen of the gastrointestinal tract, which will allow for the drainage to occur into the gastrointestinal lumen directly.
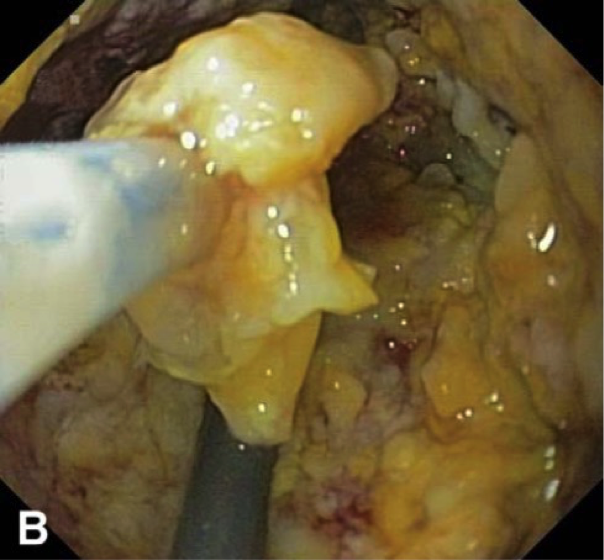
Pancreatic Necrosectomy
Sometimes after stent placement, the material in the collection gels together to become solid, in which case drainage cannot occur through the stent. For these patients, we offer the ability to perform necrosectomy, which involves taking a standard endoscopy scope and advancing it through the stent into the collection, at which point solid debris can be grabbed and removed by hand. This is an arduous task, and in some cases takes many sessions to see improvement, but is worth it in the end because only after removal of the solid material will the collection heal.
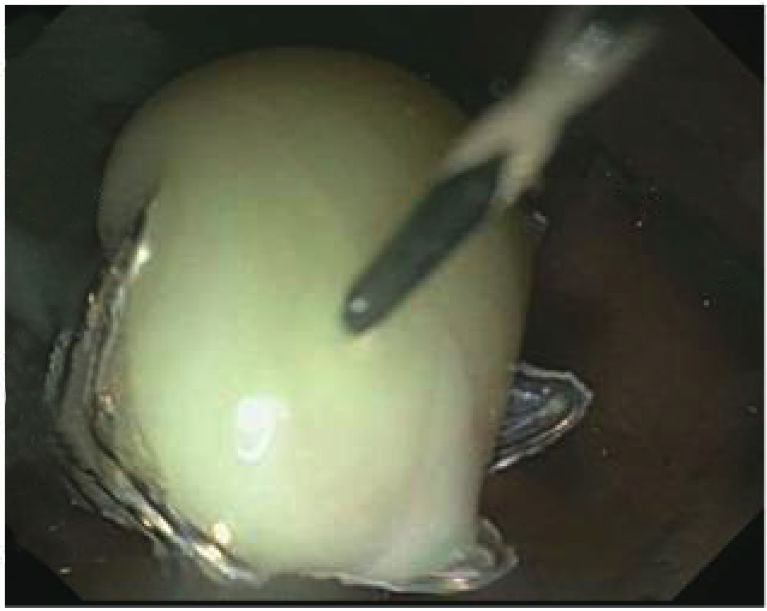
EUS-guided gallbladder drainage
When there is an obstruction in the gallbladder, the bile that is stored there is unable to drain. This leads to distension of the gallbladder, causing pain and acting as a breeding place for infection. Whenever possible, the gold standard treatment is removal of the gallbladder via surgery. However, there are many patients who are not able to undergo surgery due to age, concurrent medical conditions, severity of illness, etc. Traditionally, the only alternative for those patients was a drain from the skin into the gallbladder, left in place indefinitely. However, now we have the option to drain the gallbladder from the inside. This is done by seeing the gallbladder via endoscopic ultrasound and placing a stent from the gallbladder into the stomach or small intestine.
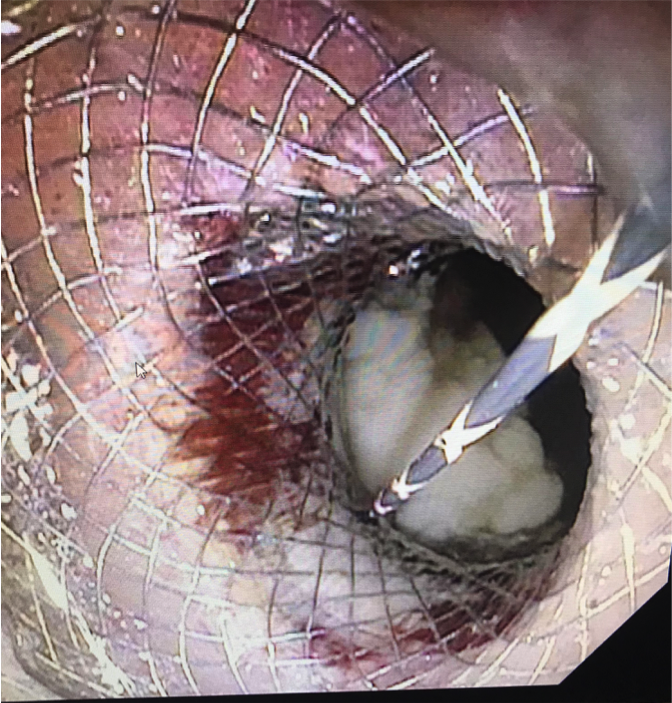
EUS-guided biliary and pancreatic duct drainage
Patients with obstruction of the bile duct or pancreatic duct require a procedure called Endoscopic Retrograde Cholangiopancreatography (ERCP). This procedure involves accessing these ducts through their normal connection point to the intestine in order to remove the obstructing agent. Sometimes a stent is placed as access to the area of obstruction. However, a small percentage of patients cannot have the blockage relieved with standard ERCP. The alternative for these patients used to be surgical intervention or placement of a drainage catheter from the skin into the ducts. However, now we have the technical skill and capability at RWJUH to drain these ducts from the inside. This involves making a new connection from the stomach or small intestine into the bile duct or pancreatic duct and placing a drainage stent across the new connection.
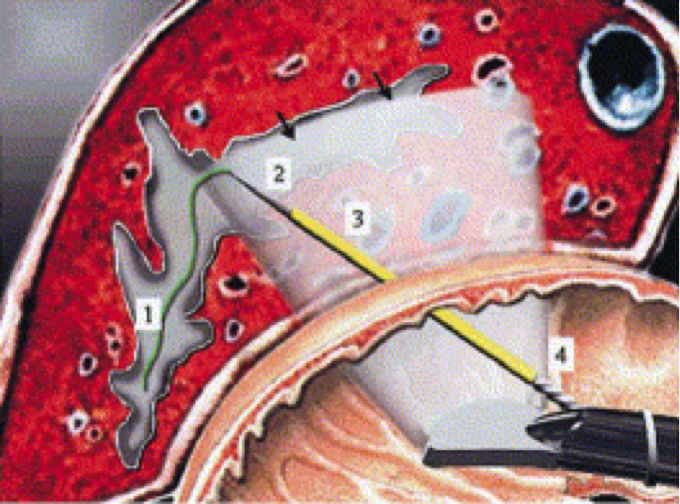
Burmester E: Gastrointest Endos 2003
EUS-Directed Transgastric ERCP (EDGE)
Gastric bypass is growing in popularity as an effective treatment for obesity. However, the procedure involves re-routing of the gastrointestinal lumen, resulting in the bile duct-intestinal anastomosis to be very far away from the gastrointestinal lumen. This is problematic for patients who develop gallstones after gastric bypass, as it is very difficult to access the bile duct in order to remove the stones. Consequently, the "EDGE" procedure was invented to overcome this difficulty. This procedure involves connecting two areas of the gastrointestinal lumen by placing a stent between the native and bypassed stomachs under endoscopic ultrasound, in other words creating a bridge to shorten the distance to the ampulla and allow for stone removal.
Endoscopic Retroperitoneal Pancreatic Necrosectomy
EUS-guided Gastrojejunostomy
Sometimes, diseases of the gastrointestinal tract cause obstruction of the stomach, preventing the passage of food from the stomach into the intestine. Surgery to re-route the intestines is an option for these patients. However, recently a minimally invasive endoscopic alternative was developed, which allows for bypassing of the obstruction—all from the inside. This procedure involves identifying the small intestine beyond the area of blockage, and placing a stent from there into the stomach. This allows patients to continue to eat and avoids the need for an invasive operation.